There aren't really any good sources for the definition of abdominal epilepsy, given that it's a diagnosis that isn't commonly accepted in neurology circles and it doesn't appear in authentic medical dictionaries, so in trying to come to your side of the fence for a while, I had to use WebMD. Here is what abdominal epilepsy is said to be:
Abdominal epilepsy is an exceptionally rare syndrome of epilepsy that's more likely to occur in children. With abdominal epilepsy, seizure activity causes abdominal symptoms. For example, it may cause pain and nausea. Anticonvulsant medications can improve the symptoms.
Abdominal epilepsy is so uncommon that some experts question whether it exists.
http://www.webmd.com/epilepsy/guide/abdominal-epilepsy-in-children-and-adults
All the definitions I find say the same thing: The focus in the brain causes the gastrointestinal symptoms, and anticonvulsants (which act on the brain) are effective in treating it. The same is seen in your papers.
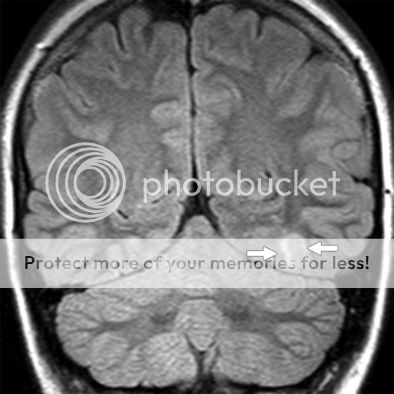
This is what a seizure focus looks like. As you can see, it is in the brain, and not the gut.
You've misunderstood the meaning of abdominal epilepsy. Abdominal epilepsy does not add to your premise. HOWEVER, if it's abdominal epilepsy that you're talking about in this thread, you're speaking about an exceptionally rare syndrome, and not about the sort of epilepsy most epilepsy patients have. If you are talking about abdominal epilepsy, you should say so in your signature so that the rest of us, and most of CWE, are aware that what you're discussing doesn't apply to us.
The brain affects the autonomic functions of the body (digestion, blood pressure, core body temperature etc). It does have an impact, in other words, on digestion. That doesn't mean that a seizure can immediately cause gastrointestinal symptoms, but it does mean that the brain can, in the case of autonomic neuropathy, cause diarrhea. It does not mean that diarrhea can cause neuropathy, or seizures.
In other words, the papers you've linked to say that the epileptic brain is causing the problem. The gut is not causing the problem. If they were decent papers, they would disprove your premise.
But it is important to remember that not all science is equal. Cherrypicking research that confirms your bias–that’s not science. Giving equal weight to everything that is written–that’s not science. Thinking that a researcher is an expert because they have a degree or qualifications in another area–that’s not science.
And these aren’t up for debate, because there is no debate, unless someone thinks that undue weight, given to bad science, is considered important evidence.
It’s important to remember that just because the science doesn’t support your point of view doesn’t mean it’s wrong. It means your point of view is wrong.
The TL;DR version:
Only high quality articles, published in peer reviewed, high impact factor scientific journals count in a discussion about science.
Expertise matters, and it’s not self-proclaimed nor is it established by a few letters after your name. It’s established by the amount and depth of respect from peers.
Not all science is equal. And the best research is a systematic review which shows a clinically significant effect.
Giving false balance or undue weight to fringe beliefs that are unsupported by the vast breadth of research in that area is inappropriate and can be ignored.
http://www.skepticalraptor.com/skepticalraptorblog.php/how-evaluate-quality-scientific-research/
This is going to sound snarky, but it's actually a question I'd really like you to answer.
Please do comment. You don't answer most of questions in this thread, so I've made the questions red to make it clear which questions I'm asking you. I'm also asking that you answer them in words and not studies, please. You're free to add studies to support your case, but simply copying and pasting a bunch of studies is not really answering a question. :
When I almost drowned as a toddler, and got epilepsy as a result, how did the near drowning affect my gut in those two minutes, in order to affect my brain, giving it a seizure focus, in order to cause seizures for the rest of my life? Did the lack of oxygen have no effect on my brain, but a rather dramatic effect on my gut. In those two minutes, did my gut microbial balance go out of whack, or become leaky, or whatever, and then did that effect travel up to my brain and carve out my seizure focus? Or did the lack of oxygen damage my brain and give me a seizure focus?
Or, more simply, (and please answer this too) in our member who got epilepsy from surgery, when the doctors cut into his brain, did his gut go out of whack as a result, and cause an effect on the brain such that a scar was formed exactly where the surgeon's scalpel was cutting, giving him epilepsy? Or did the surgeon's cutting cause a scar that gave him epilepsy?